
Sunday, 23 September 2012
Thursday, 13 September 2012
ANTENATAL CARE (ANC)
AIMS
To prepare female mentally and physically for physiological changes during pregnancy ,delivery and to keep them fit in the role of parents.
To prepare the perspective parents for the birth and care of the baby for parenthood.
To motivate,council and guide them to increase their confidence.
Provide them a forum for the perspective parents to meet each other and discuss aspects of hopes,fears,problems, and expectations.
EXERCISES AND ERGONOMICS
EXERCISE TO MAINTAIN PROPER POSTURE AND TO AVOID POSTURAL PROBLEMS LIKE PIVD,LOW BACK PAIN,ROUNDED SHOULDER etc.
Back care and lifting in various positions:-
STANDING :
Stand and walk straight,strecth head up out of shoulder.to check your posture is correct or not lean back against a wall.
Do ankle pumps to keep circulation good and ease muscle tension.
SITTING :
As spinal structures have to undergo many pressures during pregnancy its care is important .while sitting for long time into the chair place a small cushion or a pillow behind the low back as to maintain the lumbar curve and to reduce the srtecth on the posterior spinal structures.foot should be rested on floor .
SLEEPING POSITIONS :
while getting up from lying position turn to side lying and then should get up to avoid abdominal strain from sitting up or lying straight down.for most women supine from prone is acceptable as the weight of the body is taken on the bed,with a pillow placed under the abdomen and another beneath the knee.
LIFTING ADVICE :
When lifting from the floor ,it is important to ensure that the weight is light enough to be filled comfortably and not to bend from back, bend from knee.
To prepare female mentally and physically for physiological changes during pregnancy ,delivery and to keep them fit in the role of parents.
To prepare the perspective parents for the birth and care of the baby for parenthood.
To motivate,council and guide them to increase their confidence.
Provide them a forum for the perspective parents to meet each other and discuss aspects of hopes,fears,problems, and expectations.
EXERCISES AND ERGONOMICS
EXERCISE TO MAINTAIN PROPER POSTURE AND TO AVOID POSTURAL PROBLEMS LIKE PIVD,LOW BACK PAIN,ROUNDED SHOULDER etc.
Back care and lifting in various positions:-
STANDING :
Stand and walk straight,strecth head up out of shoulder.to check your posture is correct or not lean back against a wall.
Do ankle pumps to keep circulation good and ease muscle tension.
SITTING :
As spinal structures have to undergo many pressures during pregnancy its care is important .while sitting for long time into the chair place a small cushion or a pillow behind the low back as to maintain the lumbar curve and to reduce the srtecth on the posterior spinal structures.foot should be rested on floor .
SLEEPING POSITIONS :
while getting up from lying position turn to side lying and then should get up to avoid abdominal strain from sitting up or lying straight down.for most women supine from prone is acceptable as the weight of the body is taken on the bed,with a pillow placed under the abdomen and another beneath the knee.
LIFTING ADVICE :
When lifting from the floor ,it is important to ensure that the weight is light enough to be filled comfortably and not to bend from back, bend from knee.
ANKYLOSING SPONDYLITIS
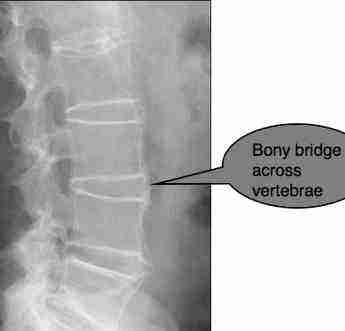
Ankylosing spondylitis mostly occurs in males,affects the axial and spinal skeleton with stiff spine,painfull back and x-ray shows typical bomboo spine structure which is important in diagnosis of disease.It is a variant type of RA.It is an inflammatory disease of spine.Inflamation of spinal synovial joints progressing to ankylosis.SACRO-ILLIATES lesion is seen.
CLINICAL FEATURES :-
1) general malaise
2) pain in -shoulder joint (with involvement of AC joint),
-jaws(with involvement of TMJ),
-over insertion of TA (due to enthesitis)
-chest region(due to sternoclavicular,costo-vertebral and costo- sternal joints involvement
3) painful breathing movements of thorax leading to reduced chest expansion
4) limited shoulder ROM due to pain and muscle spasm
5) reduced lumbar flexion and thoracic rotation
6) flattening of lumbar curve due to weakness of lumbar paraspinal muscles and
sacro-illiac involement
7) gradually progressing thoracic kyphosis
8) hip flexion deformity
9) HLA B-27 positive
PHYSIOTHERAPY MANAGEMENT :-
GOALS:- is to relieve pain,assist resolution of inflammation,prevention of deformities,maintaining spinal mobility,maintaining chest expansion,posture correction and maintaining functional independency of patient.
http://www.healthline.com/health/ankylosing-spondylitis/effects-on-body
Tuesday, 11 September 2012
FROZEN SHOULDER
Frozen shoulder, or adhesive capsulitis, is characterized by pain in the shoulder, sometimes leading into the upper arm and shoulder blade. This may cause a decrease in shoulder movement, stiffness of the shoulder joint. Frozen shoulder can be secondary to other medical problems such as thyroid illness, Parkinson disease, and cardiac disease and post-surgery. It may also be secondary to a fracture

of the shoulder or arm, tendonitis, trauma or other condition requiring shoulder immobilization for a period of time. During this time, the capsule of the shoulder joint becomes inflamed and thickened, sometimes contracted.
Patients often complain of an intense pain, dull or aching, with difficulties sleeping and a very restricted range of motion. The decrease in the range of motion decrease usually shows a pattern; some movements are more affected than others. In time this condition leads to decreased strength and stability, as well as scapular stability, and therefore reduced arm function in different degrees.
The normal course of frozen shoulder has three stages: freezing, frozen and thawing, which can last up to 2 years. Frozen Shoulder is a self-limited condition. However, physiotherapy has been proven to shorten the healing process. After assessing the physical and functional restrictions and impairments, the physiotherapist will aim the treatment towards pain and inflammation reduction, and restoration of the motion.
Only 20% of people with frozen shoulder actually have to undergo surgery. The other 80% can significantly reduce their pain if not completely abolish their frozen shoulder with exercise.
If you have a well structured exercise program you can actually find relief in 1-3 months.
There are many different treatments that people have used to combat their adhesive capsulitis; however the 'best' treatment is to make sure the patient uses frozen shoulder exercises which take advantage of a multi-level protocol.
Using a multi-level treatment protocol means that the person is not focusing on one aspect only of dealing with the problems and symptoms, rather that they are dealing with all of the issues associated with their frozen shoulder. Treatments such as this will help cover all of the bases and allow proper motion, flexibility, strength and pain reduction, which will make certain that your shoulder pain will be treated and eliminated much faster than not.
To have true success is treating adhesive capsulitis, the patient must be sure to include a good, quality stretching protocol, as well as increasing strength, treating soft-tissue issues, and working on increasing range of motion in all directions.
Patients often complain of an intense pain, dull or aching, with difficulties sleeping and a very restricted range of motion. The decrease in the range of motion decrease usually shows a pattern; some movements are more affected than others. In time this condition leads to decreased strength and stability, as well as scapular stability, and therefore reduced arm function in different degrees.
The normal course of frozen shoulder has three stages: freezing, frozen and thawing, which can last up to 2 years. Frozen Shoulder is a self-limited condition. However, physiotherapy has been proven to shorten the healing process. After assessing the physical and functional restrictions and impairments, the physiotherapist will aim the treatment towards pain and inflammation reduction, and restoration of the motion.
Only 20% of people with frozen shoulder actually have to undergo surgery. The other 80% can significantly reduce their pain if not completely abolish their frozen shoulder with exercise.
If you have a well structured exercise program you can actually find relief in 1-3 months.
There are many different treatments that people have used to combat their adhesive capsulitis; however the 'best' treatment is to make sure the patient uses frozen shoulder exercises which take advantage of a multi-level protocol.
Using a multi-level treatment protocol means that the person is not focusing on one aspect only of dealing with the problems and symptoms, rather that they are dealing with all of the issues associated with their frozen shoulder. Treatments such as this will help cover all of the bases and allow proper motion, flexibility, strength and pain reduction, which will make certain that your shoulder pain will be treated and eliminated much faster than not.
To have true success is treating adhesive capsulitis, the patient must be sure to include a good, quality stretching protocol, as well as increasing strength, treating soft-tissue issues, and working on increasing range of motion in all directions.

CARDIAC REHABILITATION
INPATIENT PHASE
TOTAL DURATION :-6-14 DAYS
1 to 7 in ICCU and 8 - 14 in the wards.
Need to maintain ROM of all joint and to avoid problems associated with orthostatic hypotension and thromboembolism.
Before starting the rehabilitation program evalaution and patients education is necessary.All viatls should be stable.Any change in systolic and diastolic pressure during exercise.systolic drop greater than 10mmHg or increase in pressure greater than 30 mmHg immediately stop the exercise.Check for HR changes and complaints like dizzeness,sightedness or angina.
Haemodynamic monitering necessary before and after exercises.
LEVEL 1:-1.5 METs
Essentially Bed rest and bed exercises.
Arm movement and ankle pumps.
Introduction and education of cardiac rehabilitation program.
SLR,heel slides.
LEVEL 2:-1.5-2 METs
Limited Room Abulation activities are allowed.
Sitting 15 - 30 min ,2-4 times /day.
Leg exercise -ankle pumps,SLR,heel slides.
Knee extention in sitting,sit to stand.
ADLs like shaving,ambulation til toilet attached to room.
Identification of CAD risk factors.
LEVEL 3:-2-2.5 METs
Limited Hall Ambulation are allowed
Independent or assisted walking continue slowly upto 5 mins are allowed for 3-4 times a day.
Continuining the bed exercise and ADL.
Bathroom privileges allowed.
Borg's scale used by P.T. for rating of Perceived Exertion and appropriate parameters with activity.
LEVEL 4:-2.5-3 METs
Progressive Hall Ambulation
Walking for 5-7 min as tolerated 3-4 times /day.
Standing trunk exercises optimal.
Reinforce benefits of outpatient cardiac rehabilitation.
LEVEL 5:-3-4 METs
Hall ambulation 8-10 min as tolerated.
Arm exercises optional.
Limeted stair climbing .
LEVEL 6:- 5 METs
Stair climing progressive .
OUTPATIENT PHASE
After discharge patient are allowed to go to home and to do ADLs and progressive exercises but before discharge patient has to undergo a low level graded exercise test which are often terminated if
1)patients HR increases to 120/130 beats / min.
2)patients HR reaches to HRmax.
Patient are allowed to do exercise to 60% to its HRmax and adviced not to do atatic,exertive,isometric activities and to take adequate rest and to follow proper diet.
Till the 6 weeks after discharge the phase is conditioning phase.
Till 3 months after discharge its convalescent phase which is a phase of improvement during which exsercise level is gradually increased
After about 6 weeks patient has to follow and undergo ETT and SL-GXT.
The last phase is the maintaining phase which starts mostly after 6 months after discharge.
TOTAL DURATION :-6-14 DAYS
1 to 7 in ICCU and 8 - 14 in the wards.
Need to maintain ROM of all joint and to avoid problems associated with orthostatic hypotension and thromboembolism.
Before starting the rehabilitation program evalaution and patients education is necessary.All viatls should be stable.Any change in systolic and diastolic pressure during exercise.systolic drop greater than 10mmHg or increase in pressure greater than 30 mmHg immediately stop the exercise.Check for HR changes and complaints like dizzeness,sightedness or angina.
Haemodynamic monitering necessary before and after exercises.
LEVEL 1:-1.5 METs
Essentially Bed rest and bed exercises.
Arm movement and ankle pumps.
Introduction and education of cardiac rehabilitation program.
SLR,heel slides.
LEVEL 2:-1.5-2 METs
Limited Room Abulation activities are allowed.
Sitting 15 - 30 min ,2-4 times /day.
Leg exercise -ankle pumps,SLR,heel slides.
Knee extention in sitting,sit to stand.
ADLs like shaving,ambulation til toilet attached to room.
Identification of CAD risk factors.
LEVEL 3:-2-2.5 METs
Limited Hall Ambulation are allowed
Independent or assisted walking continue slowly upto 5 mins are allowed for 3-4 times a day.
Continuining the bed exercise and ADL.
Bathroom privileges allowed.
Borg's scale used by P.T. for rating of Perceived Exertion and appropriate parameters with activity.
LEVEL 4:-2.5-3 METs
Progressive Hall Ambulation
Walking for 5-7 min as tolerated 3-4 times /day.
Standing trunk exercises optimal.
Reinforce benefits of outpatient cardiac rehabilitation.
LEVEL 5:-3-4 METs
Hall ambulation 8-10 min as tolerated.
Arm exercises optional.
Limeted stair climbing .
LEVEL 6:- 5 METs
Stair climing progressive .
OUTPATIENT PHASE
After discharge patient are allowed to go to home and to do ADLs and progressive exercises but before discharge patient has to undergo a low level graded exercise test which are often terminated if
1)patients HR increases to 120/130 beats / min.
2)patients HR reaches to HRmax.
Patient are allowed to do exercise to 60% to its HRmax and adviced not to do atatic,exertive,isometric activities and to take adequate rest and to follow proper diet.
Till the 6 weeks after discharge the phase is conditioning phase.
Till 3 months after discharge its convalescent phase which is a phase of improvement during which exsercise level is gradually increased
After about 6 weeks patient has to follow and undergo ETT and SL-GXT.
The last phase is the maintaining phase which starts mostly after 6 months after discharge.
Thursday, 6 September 2012
PHYSIOTHERAPIST ADVICE FOLLOWING DELIVERY
Physiotherapy
advice
following hysterectomy, repair and other gynaecology operations |
Day 1 onwards
To reduce the
effects of a general anaesthetic, practise the following exercises hourly
throughout the day.
Deep breathing exercises
Be sure that you
have adequate pain relief because deep breathing could be uncomfortable.
Practise the breathing exercises sitting up in bed, supported by pillows, or
out in a chair.
Take a deep
breath in through your nose, hold for two seconds and then sigh the air out
of your mouth. Repeat four times then try to ‘huff’ the air out.
Huffing
Take a deep
breath in, then breathe out quickly and forcefully through your mouth as if
you were steaming up a window. This will help loosen any phlegm if needed.
Coughing
Circulatory exercises
These are
designed to improve circulation in your legs whilst lying in bed or sitting
in a chair.
Try to do them
exercises every hour.
Ankles
Bend and stretch
the ankles up and down firmly and quickly. Repeat 10 times.
Knees
Tighten your
thighs by pushing the backs of your knees down against the bed. Repeat five
times.
Buttocks
Tighten your
buttocks regularly to relieve pressure from your bottom. Repeat five times.
From Day 2 onwards
Start all exercises by lying with your head on a
pillow, knees bent and a shoulder- width apart, feet flat on the bed.
1. Abdominal exercise
Gently place
your hands on your lower tummy. Breathe in through your nose and as you
breathe out, gently pull your tummy away from your hands towards your back.
Feel the muscles tighten, try to hold for a count of 3 and then relax.
Breathe in and out normally.
Practice this
exercise 3 times a day. You will gradually be able to hold for longer until
you reach 10 seconds and can repeat 10 times.
2. Pelvic Tilting
Place your hands
in the hollow of your back. Tighten your tummy muscles (Exercise 1), flatten
your lower back onto your hands and tilt your bottom. Breathe normally. Hold
for three seconds and release gently.
Try to progress
this exercise by tightening your tummy muscles and also pulling up your
pelvic floor before continuing as above.
3. Knee rolling
Tighten your
tummy muscles (Exercise 1) and gently lower both knees to one side as far as
is comfortable. Bring them back to the middle and relax. Repeat to the other
side.
4. Knee bends
Tighten your
tummy muscles (Exercise 1). Keep your back flat on the bed and bend one hip
and knee up as far as is comfortable. Try to hold up to the count of 10 and
then replace the leg, so the foot is back on the bed. Repeat with the other
side.
Repeat each of
these exercises four times, three times a day, and then do more as you feel
able.
To get out of bed
Bend both knees
and roll onto your side by moving your shoulders and knees together. Push up
by pressing your upper hand down onto the bed while you lower your feet to
the floor.
Sit on the edge
of the bed and then stand by pushing up with your legs and hands.
Posture and back
care
It is very
important to be aware of your posture and to take special care for about six
weeks after your surgery. A good posture will help prevent backache.
Sitting
Sit upright in a
supportive chair, with both feet on the floor. Do not slouch. You may find it
helpful to place a small cushion or rolled towel in the small of your back to
give support. .
Standing or walking
Avoid holding
your tummy with your hands and slouching forwards. Stand upright with
shoulders back, and bottom and tummy tucked in.
Lifting
Do not lift
heavy objects. Try to pull up your pelvic floor, tighten your tummy muscles
and breathe out as you lift.
Remember to bend
your knees and keep your back straight. Hold larger objects close to your
body.
·
If you are suffering from back pain after your
operation, seek further advice from your physiotherapist.
·
If any exercises cause pain, discontinue and seek
advice from your physiotherapist.
·
Your consultant may also wish you to practise pelvic
floor exercises. If so, a separate exercise sheet is available.
Before you go home
The need for
continued pain relief at home is very individual. Please discuss this with
your nurse.
If you have any worries or concerns, please talk to the physiotherapist or nursing staff .
Advice on discharge
Exercises
Continue with
exercises taught for at least six weeks, preferably three months.
Rest
Take a daily rest on your
bed for about an hour. Continue for as long as necessary.
Walking
This is a very
valuable exercise. Try to walk for about 20 minutes at least once a day.
Hills and stairs are quite safe, but build up speed and distance gradually.
Driving
Check with your
consultant but do not expect to drive for about four or six weeks, depending
on your surgery. Make sure you can wear a seatbelt comfortably and perform
manoeuvres and an emergency stop without undue pain.
Work
You should not
expect to return to full-time work until after your post-op appointment with
your consultant (six weeks). Always get approval from your doctor to return
to work.
Sports
Also get
approval at this appointment to return to sports, swimming, aerobics etc.
Gardening
Avoid gardening
for a few weeks. Start slowly.
Sexual
Intercourse
You should
refrain from sexual intercourse for about six weeks.
Household
Activities
'Dos and don'ts'
DOS:
Independent personal hygiene; light housework, such as dusting, ironing, making drinks; washing and drying dishes; preparing light meals. Don’ts: Decorating; heavy lifting; shaking the duvet or heavy bedding; cooking a large meal using the oven; heavy housework.
Take things
slowly. Be very careful for the first six weeks after your operation.
Gradually build up activity over the next six weeks until you feel able to resume your normal
lifestyle.
|
Theoretical Approach “Living concept”
Where
Bobath Began
|
·
Problem-solving approach based on reflex/hierarchical
models.
|
·
Hierarchical model of CNS structure and function.
|
·
CNS viewed as the “controller”. Automatic postural
control mechanism simplified the responsibility of the CNS in control of
movement.
|
·
Sensory feedback is important for the correction of
movement errors.
|
·
“Positive signs” including spasticity and abnormal
coordination of movement are the most important aspects of sensorimotor
impairments.
|
·
Muscle and postural tone determine the quality of the
patterns of posture and movement used in functional activities.
|
Where NDT Is Now
|
· Problem-solving approach based on a
system/selectionist model.
|
· Distributed model of CNS structure and function.
|
· The CNS determines the pattern of neural activity
based on input from multiple intrinsic systems and extrinsic variables that
establish the context for movement initiation and execution.
|
· Sensory feed-forward and feedback are equally
important for different aspects of movement control.
|
· The “negative signs’, including weakness,
impaired postural control and paucity of movement are recognized as equally
important as the “positive signs” in limitations of function limitations of
function.
|
· Task goals, experience, individual learning
strategies, movement synergies, energy and interests all affect the quality
of the final action.
|
Wednesday, 5 September 2012
JALGAON DISTRICT OT-PT ASSOCIATION
A golden day in the history of jalgaon physiotherapists-
FINALLY SET
"JALGAON DISTRICT OT-PT ASSOCIATION" on september 2012 with Dr.Jaywant Nagulkar(PT) as "PRESIDENT"
and Dr.NEHA INGALE(PT) elected as a "VICE PRESIDENT" of the association.
This association will work best for the awareness and upliftment of the physiotherapist profession in india and focussing on the rural areas of maharashtra .
Subscribe to:
Posts (Atom)